 On the Case
On the Case
By Racquel Helsing, MD; Christina Metcalf, MD; and Alex Merkulov, MD
Radiology Today
Vol. 25 No. 5 P. 28
History
A 27-year-old woman with no significant past medical history presented to her outpatient physician for a bothersome left nipple lesion. The lesion initially developed two years prior but had recently grown slightly in size, becoming increasingly symptomatic with pain, bleeding, and flaking of the overlying skin. She denied any trauma to the area prior to the initial appearance of the lesion. The physical exam revealed a 7-mm hypertrophic smooth nodule on the nipple at the 11 o’clock location, which demonstrated fissuring and bleeding with manipulation and blanching of the overlying skin and no sign of infection. Ultrasound and breast MRI examinations were performed to determine the extent of disease, and the patient was referred for a consultation with breast surgery.
Findings
Targeted left breast ultrasound of the nipple and of the retroareolar breast demonstrated a nonspecific parallel 8-mm hypoechoic mass centered within the nipple (Figure 1).

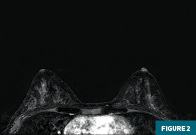
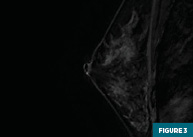
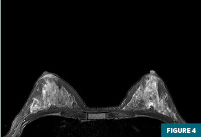
Axial and sagittal T1 postcontrast subtracted MRI images demonstrated a peripherally enhancing mass centered within the nipple with normal subareolar morphology (Figures 2 and 3). This nipple lesion was circumscribed and hyperintense on the T2 fat-saturated ASPIR axial MRI sequence (Figure 4).
The patient underwent a surgical excision of the left nipple lesion without complications.
Diagnosis
Left nipple adenoma
Discussion
Nipple adenomas represent a relatively rare but clinically significant entity in the realm of breast pathology. These benign proliferations arise from the ductal epithelium of the nipple, often presenting with various clinical manifestations and histological features. Despite their benign nature, nipple adenomas can pose diagnostic challenges, necessitating a comprehensive understanding of their clinical presentation, imaging characteristics, and histopathological features for accurate diagnosis and appropriate management.
Nipple adenomas typically manifest with symptoms such as nipple discharge, palpable masses, or nipple retraction. Although they predominantly affect women, cases have been reported in men, as well. Nipple discharge, often bloody or serous, is a common presenting complaint and may be spontaneous or provoked. However, it is essential to recognize that not all nipple adenomas present with discharge, and some may remain clinically silent, discovered incidentally on imaging or during surgical excision for unrelated concerns.
Radiological evaluation plays a crucial role in the diagnosis and characterization of nipple adenomas. Mammography and ultrasound are commonly employed modalities, with MRI occasionally utilized for further assessment in complex cases. On mammography, nipple adenomas may present as focal asymmetries, ill-defined masses, or architectural distortion involving the nippleareolar complex. Ultrasound typically reveals hypoechoic or complex masses within the subareolar region, often exhibiting irregular borders and posterior acoustic shadowing. These findings, although suggestive, lack specificity and may overlap with other benign and malignant entities, emphasizing the importance of histopathological confirmation.
Histologically, nipple adenomas exhibit a spectrum of morphological patterns, including tubular, papillary, solid, and sclerosing variants. These lesions are characterized by proliferation of ductal epithelial cells with varying degrees of atypia, supported by fibrovascular stroma. Immunohistochemical staining may demonstrate positivity for epithelial markers such as cytokeratins and epithelial membrane antigen, further aiding in their differentiation from malignant lesions. Despite their benign nature, certain histological features, such as prominent atypia or complex architecture, may raise concern for concurrent or precursor malignancy, necessitating close pathological evaluation.
The differential diagnosis of nipple adenomas encompasses a broad spectrum of benign and malignant entities, including intraductal papillomas, papillary carcinomas, ductal adenomas, and Paget’s disease of the nipple. Clinical correlation, radiological findings, and histopathological assessment are essential for accurate differentiation, as misdiagnosis may lead to inappropriate management decisions and unnecessary patient anxiety.
Given their benign nature, most nipple adenomas can be managed conservatively with close clinical surveillance. However, symptomatic lesions or those causing diagnostic uncertainty may warrant surgical excision for definitive diagnosis and treatment. The extent of excision depends on the clinical presentation, radiological findings, and pathological characteristics of the lesion, with complete resection often recommended to alleviate symptoms and mitigate the risk of recurrence. Wider excision may be warranted for malignant lesions identified on excisional biopsy.
Nipple adenomas represent a distinctive entity in the spectrum of benign breast lesions, characterized by their unique clinical presentation, imaging features, and histopathological findings. While typically benign, these lesions can mimic malignant processes both clinically and radiologically, underscoring the importance of a multidisciplinary approach involving clinicians, radiologists, and pathologists for accurate diagnosis and appropriate management. Further research into the natural history and optimal management strategies of nipple adenomas is warranted to refine current diagnostic and therapeutic algorithms and improve patient outcomes.
Racquel Helsing, MD, is a radiology resident at UConn Health at the University of Connecticut in Farmington.
Christina Metcalf, MD, is the director of breast surgery at Saint Francis Hospital in Hartford, Connecticut.
Alex Merkulov, MD, is an associate professor of radiology at UConn Health.
Resources
1. Dalal YD, Trivedi AK, Panchal V, Patel Y, Dalal DD. Nipple adenoma: case report of a rare entity. Cureus. 2022;14(3):e22996.
2. Li M, Du J, Wang LJ, Li Z, Chen X. A case of nipple adenoma detected by sonography. Chin Med J (Engl). 2016;129(19):2386-2387.
3. Matsubayashi RN, Adachi A, Yasumori K, et al. Adenoma of the nipple: correlation of magnetic resonance imaging findings with histologic features. J Comput Assist Tomogr. 2006;30(1):148-150.
4. Tatterton MR, Fiddes R. Nipple adenoma: a review of the literature. Ann Breast Surg. 2019;3:29.
5. Wang C, Wang X, Ma R. Diagnosis and surgical treatment of nipple adenoma. ANZ J Surg. 2015;85(6):444-447.