 Billing and Coding: 2025 Coding Update
Billing and Coding: 2025 Coding Update
By Melody W. Mulaik, MSHS, CRA, RCC, RCC-IR, CPC, COC, FAHRA
Radiology Today
Vol. 26 No. 1 P. 6
As we step into 2025 there is a lot of discussion around the new MR safety codes. While these codes are likely the biggest splash for 2025, there are other new codes and guidelines that should be reviewed for appropriate coding and charge capture. This article provides a high-level overview of the radiology coding updates for 2025. There may be other updates that are relevant to your organization, so it is important to review all 2025 updates.
MR Safety Codes
Six new codes 76014–76019 have been established to report MR safety: Implant and/or foreign body assessment, safety determination, medical physics examination, customization planning and performance monitoring, electronics preparation, and implant positioning and/or immobilization. A new subheading, MR Safety Implant/Foreign Body Procedures, within the Radiology/Diagnostic Radiology (Diagnostic Imaging) section has been added to the 2025 CPT codebook, providing instructional guidelines and parenthetical notes. This new subsection describes the work of reviewing records and the medical decision making that is required when assessing implanted medical devices or foreign bodies in patients who may require an MR exam for either diagnostic or interventional reasons.
Following are the new codes and a high-level overview of the guidelines. Detailed guidance should be reviewed if you have any questions or concerns regarding how your providers or staff documents and bills for these services (see Chart 1).

Codes 76014–76016 represent preprocedure assessment services. Codes 76014–76015 are typically performed by technologists and do not include independent decision making. They describe MR safety-planning services performed in advance of the date of the MR procedure, except for same day emergent circumstances. The first two codes, 76014–76015, do not require physician work or a formal written report. These codes describe documentation by a technologist or other MR safety-trained clinical staff of MR conditions, contraindications, and adherence to instructions for equipment and personnel scheduling.
Code 76014 is reported for the initial 15 minutes of preprocedure assessment by trained clinical staff. Note that American Medical Association (AMA) guidelines require that only the halfway point of time be achieved so a minimum of eight minutes must be performed and documented. Code 76015 is available to report each additional 30 minutes (so minimum 16+ minutes) required to complete the assessment for patients that have complex, multiple, or incompletely documented implants. Code 76015 is an add-on code that can only be reported three times per encounter, in conjunction with its parent code, 76014. As with all time-based codes, the exact time spent to perform the defined services must be documented in the medical record.
Code 76016, requires physician work and a written report and should be assigned only when an implant and/or foreign body lacks MR conditional labeling, is contraindicated for MR, or may result in a limited MR examination based upon the performance of an MR safety determination by a physician or other qualified health care professional (QHP) responsible for the safe performance of the MR procedure. As a reminder, a qualified health care professional is defined by the AMA as an individual who is qualified to bill for the defined services under their own name/number.
Codes 76017–76019 describe MR safety services performed on the day of the MR examination under supervision of the physician or other QHP responsible for the safe performance of the MR procedure. The need for these services depends on the design of the medical implant, and the MR conditional labeling of the implant (if available). All of these codes require a written report.
These same day services (codes 76017–76019) are typically performed in addition to the previously discussed services performed prior to the date of service of the MR examination (codes 76014–76016); however, the same day services (codes 76017–76019) may also be performed as stand-alone services.
If an implant requires electronics preparation or positioning and/ or immobilization prior to the MR, procedure codes 76018 and 76019 may be reported in conjunction with code 76017 for the medical physics services.
Code 76018 is intended to report preparation and documentation of an electronic implant into an MRprotective mode. Cardiac devices (eg, pacemakers and defibrillators) may require interrogation or programming services before or after the performance of an MR exam, to put them in a mode that is safe for the MR scan. Similarly, the same analysis programming applies to neurostimulation devices. If a cardiac device and a neurostimulation device require interrogation or programming services on the same day, only one unit of 76018 should be reported if the same individual performs both MR safety services. If each MR safety service is performed by separate individuals, then two units of 76018 may be assigned.
Code 76018 may be reported in conjunction with 76017 when the implant also requires medical physics examination customization.
Code 76019 is intended to report specified positioning and/or immobilization of an implant during the MR examination, with documentation for inclusion in the medical record. When the implant also requires medical physics examination customization, code 76019 should be reported in conjunction with 76017.
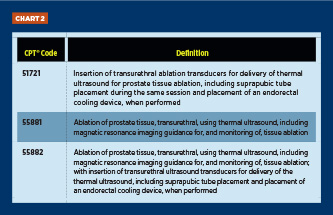
MRI – Monitored Transurethral Ultrasound Ablation (TULSA)
Three new codes were created for the TULSA procedure which delivers predictable physician-prescribed ablation of prostate tissue for treatment of prostate cancer. The first code is assigned if a physician only inserted the transducer, which would typically be a urologist. The second code is assigned if the only service provided by the physician was the ablation, which would typically be an interventional radiologist. The third code represents the complete procedure where the physician performs the entire service, which could be either a urologist or an interventional radiologist (see Chart 2).
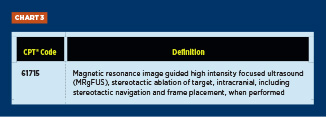
MRI-Guided High Intensity Focused Ultrasound
The existing Category III code 0398T was slightly modified into a new Category I code with the following definition (see Chart 3):
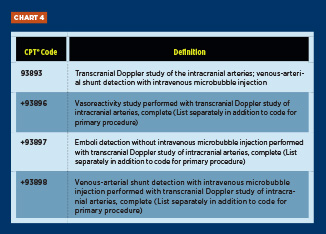
Transcranial Doppler
The Cerebrovascular Arterial Studies guidelines in the CPT codebook were revised to clarify when existing transcranial Doppler study codes and the three new add-codes (93896–93898) could be reported. In addition to the new codes, the existing code 93893 (Transcranial Doppler study of the intracranial arteries; emboli detection with intravenous microbubble injection) was revised to describe venousarterial shunt detection.
Codes 93896–93898 were created to report procedures performed with a complete transcranial Doppler study of the intracranial arteries (see Chart 4).
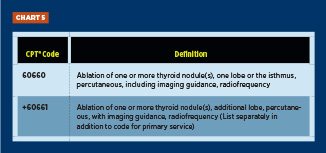
Percutaneous Radiofrequency Thyroid Ablation
Two new codes have been created to report percutaneous radiofrequency ablation of thyroid nodules. The first code represents ablation of one or more thyroid nodules in one lobe or the isthmus and includes imaging guidance. The add-on code should be assigned for ablation of one or more nodules in an additional lobe. Note that Category III code 0673T still exists for laser ablation of benign thyroid nodules (see Chart 5).
Clarification on 75774 – Each Additional Vessel Imaging
Verbiage has been added to the CPT codebook to clarify that code 75774 (Angiography, selective, each additional vessel studied after basic examination, radiological supervision, and interpretation (list separately in addition to code for primary procedure) may be reported for both arteries and veins.
Summary
Taking the time to ensure that you review all of the coding updates for a new year will ensure that you do not miss any opportunities to appropriately capture revenue for the services being performed by your radiologists. Every year brings something new, and 2025 definitely does not disappoint.
— Melody W. Mulaik, MSHS, CRA, RCC, RCC-IR, CPC, COC, FAHRA, is the president of Coding Strategies, Inc, and Revenue Cycle, Inc.
