 On the Case
On the Case
By Joseph Sisti, BS; Joseph Waller, MD; Maria Laura Gregorio, MD; and Min Chul Shin, MD
Radiology Today
Vol. 26 No. 1 P. 30
History
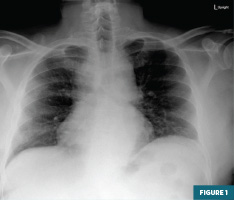
A 66-year-old man presented to the emergency department following a syncopal episode. The initial chest X-ray revealed a widened mediastinum but was otherwise unremarkable. A CT angiography (CTA) of the chest was ordered, and cardiology was consulted.
Findings
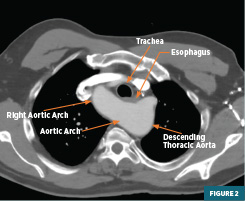
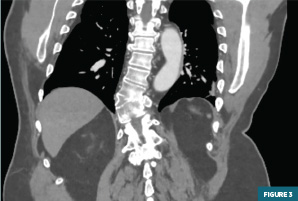
Frontal radiography of the chest demonstrated a widened mediastinum but was otherwise unremarkable (Figure 1). CTA of the chest with IV contrast in the axial plane demonstrated a right-sided aortic arch with retroesophageal crossing of the aorta to the contralateral side. These findings were consistent with a right circumflex aorta. This anatomical anomaly was associated with posterior compression of the esophagus without significant upstream esophageal dilation. The first branch arising from the aortic arch was the left common carotid artery, followed by the right common carotid artery, then by the right subclavian artery, and finally, the left subclavian artery, which originated from a small diverticulum (Figure 2). CTA of the chest with IV contrast, in the coronal plane, demonstrated the descending aorta on the left side of the patient after traveling posterior to the esophagus in the axial plane (Figure 3).
Diagnosis
Right Circumflex Aorta
Discussion
Circumflex aorta is a rare anomaly that occurs when there is retroesophageal crossing of the aorta before it descends to the contralateral side causing a vascular ring. While it is most common in patients with a right aortic arch, it can also occur with aortic arches originating from both sides. The right sided variant occurs embryologically from the regression of the left fourth branchial arch and ductus arteriosus and is associated with persistence of the dorsal aorta.1,2
A vascular ring derives as a variant of the aortic arch and its branching vessels that form a ring and compress around the trachea and esophagus. Other similar examples of anatomical abnormalities include a double aortic arch and pulmonary artery sling. The double aortic arch is the most severe and presents prior to one month of age with noisy breathing and cough. This variant can include a dominant right arch, left arch, or symmetrically balanced arches.3 A pulmonary artery sling occurs when the left pulmonary artery, which branches from the right, is posterior to the trachea and esophagus. This forms a compressive vascular ring with varying degrees of symptoms but is typically diagnosed by one year of age.4
Clinically, the circumflex aorta can present at any age and may be seen in patients with wheezing, stridor, dyspnea, dysphagia, and frequent respiratory tract infections. Most often, patients are infants and parents are concerned when noticing loud breathing and issues swallowing when solid foods are initiated in the diet. However, some patients remain asymptomatic throughout their life.5
On chest radiograph, the right circumflex aorta often appears nonspecifically as mediastinal widening from aortic knobs on either side of the aortic arch passing posteriorly to the esophagus. A barium swallow can show esophageal compression with varying degrees of severity as well as reflux into the nasopharynx in more severe cases. CTA with 3D reconstruction is confirmatory for this variant.
For the treatment of this anatomical variant, only patients with severe symptoms are indicated for an invasive uncrossing procedure due to the substantial risks associated with surgery. During the procedure, the ligamentum arteriosum is ligated while the anatomical pathology is completely resolved by the intervention.6
A circumflex aorta is especially rarely first seen in the adult population and is one that can be easily missed if only plain films are taken. Special considerations need to be taken in patients of all ages with chronic respiratory symptoms and dysphagia. In the pediatric population, it is vital to obtain imaging to confirm a vascular ring with a CTA for expedited vascular surgery interventions when indicated.
Joseph Sisti, BS, is a fourth-year medical student at Lewis Katz School of Medicine at Temple University in Philadelphia.
Joseph Waller, MD, is a postgraduate year two diagnostic radiology resident at Christiana Care in Delaware.
Maria Laura Gregorio, MD, is a staff radiologist at Christiana Care.
Min Chul Shin, MD, is a staff radiologist at Christiana Care.
References
1. Saxena S, Katewa A, Haranal M, et al. Circumflex aortic arch: presentation across various age groups: a case series. Indian J Thorac Cardiovasc Surg, 2022;38(6):624–627. https://doi.org/10.1007/s12055-022-01394-3
2. Russell HM, Rastatter JC, Backer CL. The aortic uncrossing procedure for circumflex aorta. Operative Techniques in Thoracic and Cardiovascular Surgery, 2013;18(1):15–31. https://doi.org/10.1053/j.optechstcvs.2013.03.001
3. Backer CL, Mongé MC, Popescu AR, Eltayeb OM, Rastatter JC, Rigsby CK. Vascular rings. Seminars in Pediatric Surgery. 2016:25(3);165–175. https://doi.org/10.1053/j.sempedsurg.2016.02.009
4. Lee M, Landsem L. Pulmonary Artery Sling. [Updated 2023 Jul 25]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan. https://www.ncbi.nlm.nih.gov/books/NBK562199/
5. Bader V, Knight WB, Danton MH, Peng E. Congenital arch malformation: a review of morphology and surgical management of circumflex aortic arch. Vessel Plus. 2020;4:34. http://dx.doi.org/10.20517/2574-1209.2020.36
6. Bruniaux J, Villain E, Sidi D, et al. Severe tracheo-bronchial compression caused by a circumflex aorta. Apropos of 3 cases treated by aortic uncrossing. Arch Mal Coeur Vaiss. 1984;77:557-563.
